U.S. Department of Justice Civil Rights Division Disability Rights Section |
U.S. Department of Health |
 |

Americans with Disabilities Act
Access To Medical Care For
Individuals With Mobility Disabilities

PART I: OVERVIEW AND GENERAL REQUIREMENTS
PART 2: COMMONLY ASKED QUESTIONS
PART 3: ACCESSIBLE EXAMINATION ROOMS
PART 4: ACCESSIBLE MEDICAL EQUIPMENT
Reproduction
Reproduction of this document is encouraged.
This publication may be obtained, viewed or downloaded
from the ADA Website (www.ada.gov).
Additional copies may be obtained
by calling the ADA Information Line
at
800-514-0301 (voice),
833-610-1264 (TTY).
July 2010
PART I: OVERVIEW AND GENERAL REQUIREMENTS
Accessibility of doctors' offices, clinics, and other health care providers is essential in providing medical care to people with disabilities. Due to barriers, individuals with disabilities are less likely to get routine preventative medical care than people without disabilities. Accessibility is not only legally required, it is important medically so that minor problems can be detected and treated before turning into major and possibly life-threatening problems.
The Americans with Disabilities Act of 1990 (ADA) is a federal civil rights law that prohibits discrimination against individuals with disabilities in every day activities, including medical services. Section 504 of the Rehabilitation Act of 1973 (Section 504) is a civil rights law that prohibits discrimination against individuals with disabilities on the basis of their disability in programs or activities that receive federal financial assistance, including health programs and services. These statutes require medical care providers to make their services available in an accessible manner. This technical assistance publication provides guidance for medical care providers on the requirements of the ADA in medical settings with respect to people with mobility disabilities, which include, for example, those who use wheelchairs, scooters, walkers, crutches, or no mobility devices at all.
The ADA requires access to medical care services and the facilities where the services are provided. Private hospitals or medical offices are covered by Title III of the ADA as places of public accommodation. Public hospitals and clinics and medical offices operated by state and local governments are covered by Title II of the ADA as programs of the public entities. Section 504 covers any of these that receive federal financial assistance, which can include Medicare and Medicaid reimbursements. The standards adopted under the ADA to ensure equal access to individuals with disabilities are generally the same as those required under Section 504.
Services and Facilities
Both Title II and Title III of the ADA and Section 504 require that medical care providers provide individuals with disabilities:
- full and equal access to their health care services and facilities; and
- reasonable modifications to policies, practices, and procedures when necessary to make health care services fully available to individuals with disabilities, unless the modifications would fundamentally alter the nature of the services (i.e. alter the essential nature of the services).
The ADA sets requirements for new construction of and alterations to buildings and facilities, including health care facilities. These requirements are found in the regulations for the ADA, at 28 CFR 35.151, for Title II entities and at 28 CFR Part 36, Subpart D, for Title III entities. The regulations are available at https://archive.ada.gov/regs2010/titleII_2010/titleII_2010_regulations.htm and https://archive.ada.gov/regs2010/titleIII_2010/titleIII_2010_regulations.htm.
In addition, all buildings, including those built before the ADA went into effect, are subject to accessibility requirements for existing facilities. Under Title III, existing facilities are required to remove architectural barriers where such removal is readily achievable. Barrier removal is readily achievable when it is easily accomplishable and able to be carried out without much difficulty or expense. If barrier removal is not readily achievable, the entity must make its services available through alternative methods, if those methods are readily achievable. Under Title II, a public entity must ensure that its program as a whole is accessible; this may entail removing architectural barriers or adopting alternative measures, such as relocating activities to accessible locations. This same program accessibility standard applies under Section 504.
PART 2: COMMONLY ASKED QUESTIONS
- Is it OK to examine a patient who uses a wheelchair in the wheelchair, because the patient cannot get onto the exam table independently?
Generally no. Examining a patient in their wheelchair usually is less thorough than on the exam table, and does not provide the patient equal medical services. There are several ways to make the exam table accessible to a person using a wheelchair. A good option is to have a table that adjusts down to the level of a wheelchair, approximately 17-19 inches from the floor. (See Part 4 of this publication for a more in-depth discussion of accessible exam tables.) What is important is that a person with a disability receives equal medical services to those received by a person without a disability. If the examination does not require that a person lie down (for example, an examination of the face), then the exam table is not important to the medical care and the patient may remain seated.
- Can I tell a patient that I cannot treat her because I don't have accessible medical equipment?
Generally no. You cannot deny service to a patient whom you would otherwise serve because she has a disability. You must examine the patient as you would any patient. In order to do so, you may need to provide an accessible exam table, an accessible stretcher or gurney, or a patient lift, or have enough trained staff available who can assist the patient to transfer.
- Is it OK to tell a patient who has a disability to bring along someone who can help at the exam?
No. If a patient chooses to bring along a friend or family member to the appointment, they may. However, a patient with a disability, just like other individuals, may come to an appointment alone, and the provider must provide reasonable assistance to enable the individual to receive the medical care. This assistance may include helping the patient to undress and dress, get on and off the exam table or other equipment, and lie back and be positioned on the examination table or other equipment. Once on the exam table, some patients may need a staff person to stay with them to help maintain balance and positioning. The provider should ask the patient if he or she needs any assistance and, if so, what is the best way to help.
- If the patient does bring an assistant or a family member, do I talk to the patient or the companion? Should the companion remain in the room while I examine the patient and while discussing the medical problem or results?
You should always address the patient directly, not the companion, as you would with any other patient. Just because the patient has a disability does not mean that he or she cannot speak for him or herself or understand the exam results. It is up to the patient to decide whether a companion remains in the room during your exam or discussion with the patient. The patient may have brought a companion to assist in getting to the exam, but would prefer to ask the companion to leave the room before the doctor begins a substantive discussion. Before beginning your examination or discussion, you should ask the patient if he or she wishes the companion to remain in the room.
- Can I decide not to treat a patient with a disability because it takes me longer to examine them, and insurance won't reimburse me for the additional time?
No, you cannot refuse to treat a patient who has a disability just because the exam might take more of your or your staff's time. Some examinations take longer than others, for all sorts of reasons, in the normal course of a medical practice.
- I have an accessible exam table, but if it is in use when a patient with a disability comes in for an appointment, is it OK to make the patient wait for the room to open up, or else use an exam table that is not accessible?
Generally, a patient with a disability should not wait longer than other patients because they are waiting for a particular exam table. If the patient with a disability has made an appointment in advance, the staff should reserve the room with the accessible exam table for that patient's appointment. The receptionist should ask each individual who calls to make an appointment if the individual will need any assistance at the examination because of a disability. This way, the medical provider can be prepared to provide the assistance and staff needed. Accessibility needs should be noted in the patient's chart so the provider is prepared to accommodate the patient on future visits as well. If the medical provider finds that it cannot successfully reserve the room with the accessible exam table for individuals with disabilities, then the provider should consider acquiring additional accessible exam tables so that more exam rooms are available for individuals with disabilities.
- In a doctor's office or clinic with multiple exam rooms, must every examination room have an accessible exam table and sufficient clear floor space next to the exam table?
Probably not. The medical care provider must be able to provide its services in an accessible manner to individuals with disabilities. In order to do so, accessible equipment is usually necessary. However, the number of accessible exam tables needed by the medical care provider depends on the size of the practice, the patient population, and other factors. One accessible exam table may be sufficient in a small doctor's practice, while more will likely be necessary in a large clinic. (See Part 4 for discussion of accessible exam tables and clear floor space.)
- I don't want to discriminate against patients with disabilities, but I don't want my staff to injure their backs by lifting people who use wheelchairs onto exam tables. If my nurse has a bad back, then she doesn't have to help lift a patient, does she?
Staff should be protected from injury, but that doesn't justify refusing to provide equal medical services to individuals with disabilities. The medical provider can protect his or her staff from injury by providing accessible equipment, such as an adjustable exam table and/or a ceiling or floor based patient lift, and training on proper patient handling techniques as necessary to provide equal medical services to a patient with a disability. (See Part 4 for more information on this equipment.)
- What should I do if my staff do not know how to help a person with a disability transfer or know what the ADA requires my office to do? Also, I am unsure how to examine someone with spasticity or paralysis.
To provide medical services in an accessible manner, the medical provider and staff will likely need to receive training. This training will need to address how to operate the accessible equipment, how to assist with transfers and positioning of individuals with disabilities, and how not to discriminate against individuals with disabilities. Local or national disability organizations may be able to provide training for your staff. This document and other technical assistance materials found on the ADA Website (www.ada.gov) can be used in conjunction with live training to train medical staff. The U.S. Department of Justice ADA Information Line is another resource. Anyone can call the Information Line at 800-514-0301 (voice) or 833-610-1264 (TTY) to speak with an ADA Specialist to get answers to questions about the ADA. Additionally, when preparing to assist a patient with a disability, it is always best to ask the patient if assistance is needed and if so, what is the best way to help. If the provider is unsure of how to handle something, it is absolutely OK to ask the patient what works best.
- If I lease my medical office space, am I responsible for making sure the examination room, waiting room, and toilet rooms are accessible?
Yes. Any private entity that owns, leases or leases to, or operates a place of public accommodation is responsible for complying with Title III of the ADA. Both tenants and landlords are equally responsible for complying with the ADA. However, your lease with the landlord may specify that, as between the parties, the landlord is responsible for some or all of the accessibility requirements of the space. Frequently, the tenant is made responsible for the space it uses and controls (e.g., the examination rooms and reception area), while the landlord is responsible for common space, such as toilet rooms used by more than one tenant.
- Are there any tax breaks for making accessibility changes to my medical office?
Yes. Subject to IRS rules, federal tax credits and deductions are available to private businesses to offset expenses incurred to comply with the ADA. See Form 8826 at www.irs.gov/pub/irs-pdf/f8826.pdf for additional information about the Disabled Access Credit established under Section 44 of the Internal Revenue Code. See Publication 535 (Number 7: Barrier Removal) at www.irs.gov/publications/p535/index.html for more information about the tax deduction, established under Section 190 of the Internal Revenue Code. Both the tax credit and deduction may be taken annually.
PART 3: ACCESSIBLE EXAMINATION ROOMS
Accessible examination room has features that make it possible for patients with mobility disabilities, including those who use wheelchairs, to receive appropriate medical care. These features allow the patient to enter the examination room, move around in the room, and utilize the accessible equipment provided. The features that make this possible are:
- an accessible route to and through the room;
- an entry door with adequate clear width, maneuvering clearance, and accessible hardware;
- appropriate models and placement of accessible examination equipment (See Part 4 for detailed discussion of accessible examination equipment.); and
- adequate clear floor space inside the room for side transfers and use of lift equipment.
New and altered examination rooms must meet requirements of the ADA Standards for Accessible Design. Accessible examination rooms may need additional floor space to accommodate transfers and for certain equipment, such as a floor lift.
The number of examination rooms with accessible equipment needed by the medical care provider depends on the size of the practice, the patient population, and other factors. One such exam room may be sufficient in a small doctor's practice, while more will likely be necessary in a large clinic.
Entry Doors
Under the ADA Standards for Accessible Design, an accessible doorway must have a minimum clear opening width of 32 inches when the door is opened to 90 degrees.
Maneuvering clearances on either side of the door that comply with the ADA Standards must be provided. In addition, the door hardware must not require tight twisting, pinching, or grasping in order to use it. Keep in mind that the hallway outside of the door and the space inside the door should be kept free of boxes, chairs, or equipment, so that they do not interfere with the maneuvering clearance or accessible route.
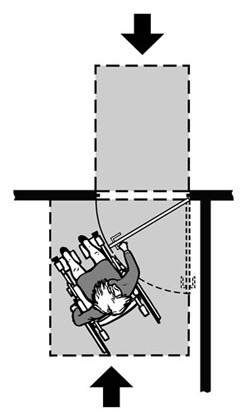
Plan view showing clear floor space on both sides of entry door to permit entry and exit
Clear Floor and Turning Space Inside Examination Rooms
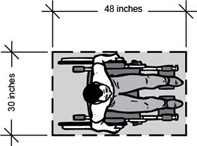
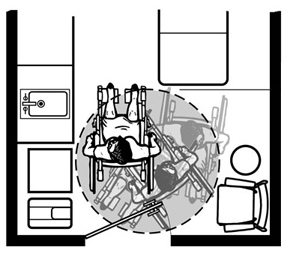
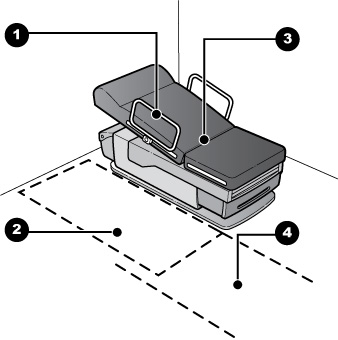
In order for accessible equipment to be usable by an individual who uses a wheelchair or other mobility device, that individual must be able to approach the exam table and any other elements of the room to which patients have access. The exam table must have sufficient clear floor space next to it so that an individual using a wheelchair can approach the side of the table for transfer onto it. The minimum amount of space required is 30 inches by 48 inches. Clear floor space is needed along at least one side of an adjustable height examination table. Because some individuals can only transfer from the right or left side, providing clear floor space on both sides of the table allows one accessible table to serve both right and left side transfers. Another way to allow transfers to either side of exam tables, particularly when more than one accessible examination room is available, is to provide a reverse furniture layout in another accessible examination room. The room should also have enough turning space for an individual using a wheelchair to make a 180-degree turn, using a clear space of 60 inches in diameter or a 60 inch by 60 inch T-shaped space. Movable chairs and other objects, such as waste baskets, should be moved aside if necessary to provide sufficient clear floor space for maneuvering and turning. When a portable patient lift or stretcher is to be used, additional clear floor space will be needed to maneuver the lift or stretcher. Ceiling-mounted lifts, on the other hand, do not require the additional maneuvering clear floor space because these lifts are mounted overhead. (See Part 4 of this publication for more information about lifts.) |
Plan view showing an outline of
Patient sitting on adjustable height exam table
Plan view of part of an examination room showing clear floor space for turning a wheelchair. This space can also make it possible for use of a portable patient lift. |

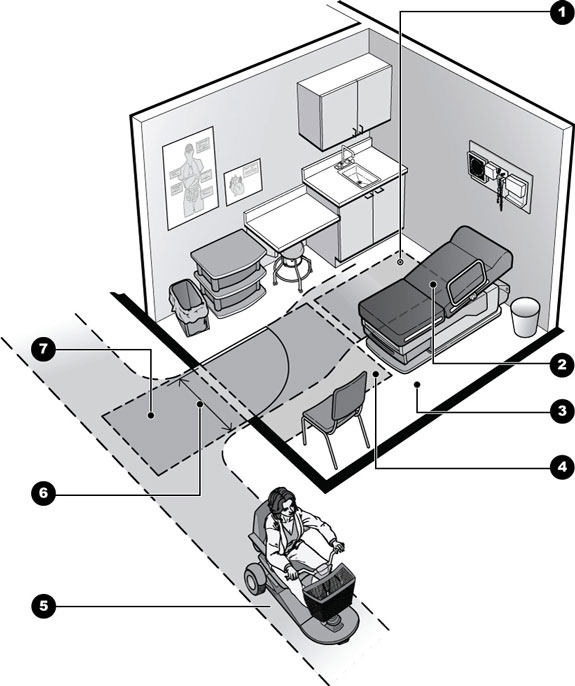
Features of an Accessible Examination Room
|
Note: Additional clear floor space can be provided by moving or relocating chairs, trash cans, carts, and other items. |
PART 4: ACCESSIBLE MEDICAL EQUIPMENT
Availability of accessible medical equipment is an important part of providing accessible medical care, and doctors and other providers must ensure that medical equipment is not a barrier to individuals with disabilities. This section provides examples of accessible medical equipment and how it is used by people with mobility disabilities. Such equipment includes adjustable-height exam tables and chairs, wheelchair-accessible scales, adjustable-height radiologic equipment, portable floor and overhead track lifts, and gurneys and stretchers.
The right solution or solutions for providing accessible medical care depends on existing equipment, the space available both within the examination room and for storage of equipment, the size of the practice and staff, and the patient population. What is important is that a person with a disability receives medical services equal to those received by a person without a disability. For example, if a patient must be lying down to be thoroughly examined, then a person with a disability must also be examined lying down. Likewise, examinations which require specialized positioning, such as gynecological examinations, must be accessible to a person with a disability. To provide an accessible gynecological exam to women with paralysis or other conditions that make it difficult or impossible for them to move or support their legs, the provider may need an accessible height exam table with adjustable, padded leg supports, instead of typical stirrups.
However, if the examination or procedure does not require that a person lie down (for example, an examination of the face or an x-ray of the hand), then using an exam table is not necessarily important to the quality of the medical care and the patient may remain seated.
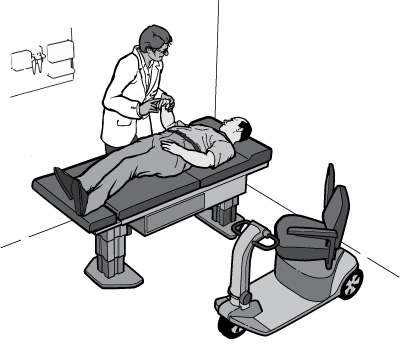
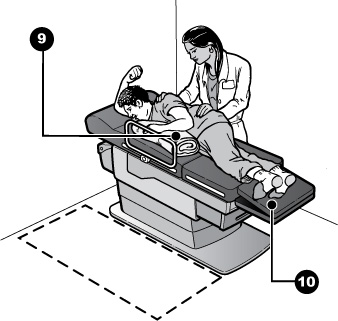
A patient with a mobility disability is
examined
while lying down on an adjustable height exam table.
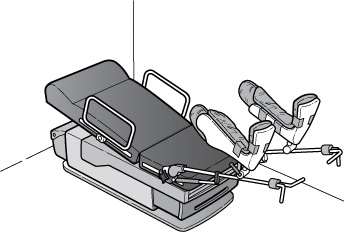
An adjustable height exam table equipped
with adjustable, padded leg supports.
Exam Tables and Chairs
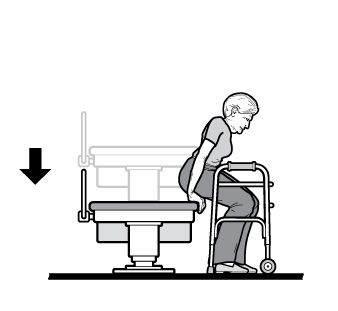
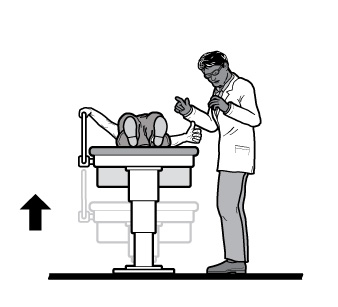
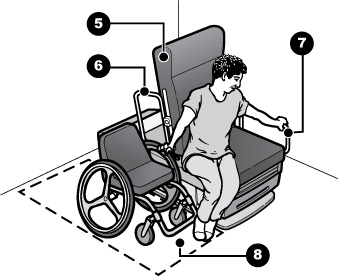
Traditional fixed-height exam tables and chairs (also called treatment tables or procedure tables) are too high for many people with a mobility disability to use. Individuals with mobility disabilities often need to use an adjustable-height table which, when positioned at a low height, allows them to transfer from a wheelchair. A handle or support rail is often needed along one side of the table for stability during a transfer and during the examination. Individuals transfer to and from adjustable-height exam tables and chairs differently. Some will be able to transfer on their own by standing up from a mobility device, pivoting, and sitting down on the exam table. Those using walkers may simply walk to the exam table and sit down, while others with limited mobility may walk more slowly and need a steadying arm or hand to help with balance and sitting down. Some people using wheelchairs may be able to independently transfer to the table or chair, while others will need assistance from a staff member. Transfers may also require use of equipment, such as a transfer board or patient lift. An accessible exam table or chair should have at least have the following:
Once a patient has transferred, staff should ask if assistance is needed -- some patients may need staff to stay and help undress or stabilize them on the table. Never leave the patient unattended unless the patient says they do not need assistance. Different types of exam tables are used for different purposes. Some exam tables fold into a chair-like position; others remain flat. Either type can be used by people with disabilities with the right accessible features and table accessories. Pillows, rolled up towels, or foam wedges may be needed to stabilize and position the patient on the table. Tilt, adjustability, and headrests, footrests, and armrests may make the examination more accessible for the patient and also easier for the doctor. |
An adjustable height exam table |
Features of Accessible Exam Tables
Click for larger image |
Click for larger image |
|
Typical Transfer Techniques: Staff Assistance and Patient Lifts
Some individuals will need additional assistance to get on and off an exam table, even if it lowers to 17-19 inches from the floor. The kind of assistance needed will depend on the patient's disability. The provider should ask the patient if he or she needs assistance, and if so, what is the best way to help and what extra equipment, if any, is needed.Some individuals will need only a steady hand from a staff person in order to transfer safely to the exam table. Other individuals will need simple tools such as a transfer board (a product made of a smooth rigid material which acts as a supporting bridge between a wheelchair and another surface, along which the individual slides) or sheet. Individuals using a transfer board may need assistance from a staff person
Assisted transfer using a transfer board and gait belt with handles

- Gait belt with handles assists with guiding along transfer board
- Transfer or sliding board acts as a bridge between wheelchair seat and table surface
Patients who can complete an independent transfer may prefer to do so for reasons of safety and simplicity.
Using Patient Lifts
Medical providers may need a lift in order to transfer some patients safely onto an exam table. Patient lifts may move along the floor or be mounted on an overhead track attached to the ceiling or to a free-standing frame. A staff person operates the lift. To use the lift, a sling is positioned under the individual while sitting in the wheelchair. Then the sling is attached to the lift so the staff person can move the individual to the examination surface. Once over the surface, the individual is lowered onto the table, stabilized, and then the sling is detached from the lift. The sling may remain under the patient during the exam or may be removed, depending on the exam. A variety of slings are available to provide different kinds of support.
Using lifts provides better security for the patient than being lifted by medical staff because there is less likelihood that the individual will be dropped or hurt in the process. Patient lifts also protect health care providers from injuries caused by lifting patients.
The most common types of lifts in medical settings are portable with a U-shaped base that moves along the floor on wheels. These bases must go under, or fit around, the exam table in order to accomplish the transfer. A lift's base may fit around the bottom end of an exam table, or fit fully or partially under the table at a perpendicular angle to the table. Some lifts are more easily operated by two or more people; others may be operated by one person. An advantage of a portable floor lift is that it can be moved from room to room and thus used with multiple exam tables. If a lift is used with multiple exam tables, the medical provider, depending on its size, may need to establish a procedure governing how the lift is shared and where it is stored. The provider should ensure that it does not schedule for the same appointment time more than one patient needing the lift. While these lifts may be less expensive than overhead lifts, they require more maneuvering space in the room and space for storage.
To properly and safely assist patients with transfers, medical staff will likely need training on how to operate the equipment and on safe patient handling techniques.
Notes for Portable Floor Lifts:
- The amount of clear floor space needed to maneuver will depend on the type of floor lift equipment used.
- Portable floor lifts must be able to position the patient over the table surface; select a model that is compatible with the exam table and room configuration.
- A low height, adjustable width base can move closer to the end of the exam table and can be narrowed for transit and storage.
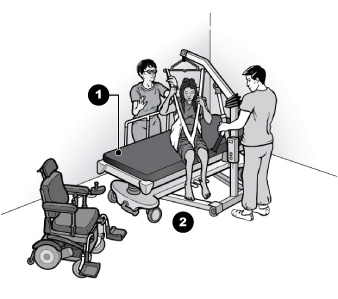
Assisted Transfer Utilizing a Portable Floor Lift

- A low height, adjustable width base permits the lift to be positioned at the end of the examination table
Assisted Transfer Utilizing Both a Portable Floor Lift and Movable Exam Table
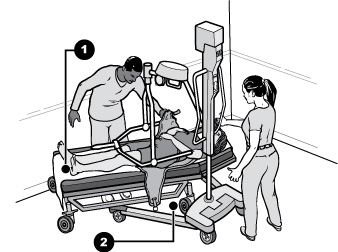
- Movable exam tables allow additional flexibility to position table and lift for optimal patient transfer
- Clearance beneath the exam table and an angled approach of the lift allows the patient to be positioned directly over the exam table for a safe transfer
Overhead Track Lifts
Overhead track lifts include ceiling mounted lifts and lifts mounted on a frame supported from the floor.
Ceiling Mounted Lifts
Ceiling mounted lifts are permanently mounted to the ceiling structure and run along one or more tracks. These lifts require no extra maneuvering space in the room adjacent to the exam table and require little storage space. However, they cannot be used in multiple exam rooms, since they are permanently attached to the ceiling structure.
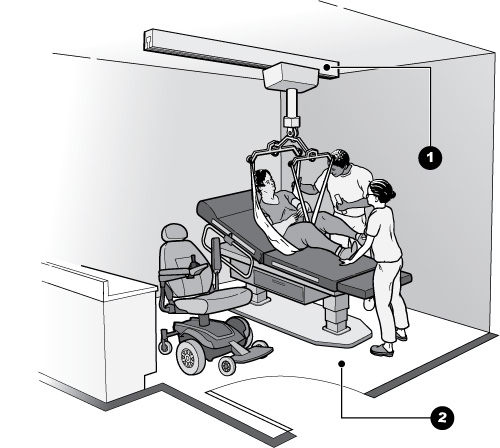
Assisted Transfer with Ceiling Mounted Overhead Track Lift
|
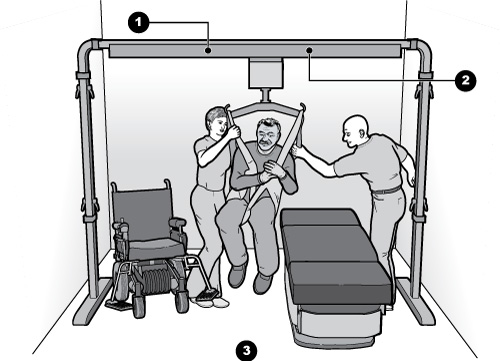
Another type of overhead lift is supported from a frame that rests on the floor. Free-standing, nonpermanent overhead track lifts are a good solution when the provider does not want the lift to be permanently installed or where the existing ceiling structure cannot support a ceiling-mounted overhead lift. The medical provider should choose the type of lift that will work best with the exam tables, the space, and the ceiling or floor structure of the medical facility.
Assisted Transfer with Free Standing Overhead Track Lift
|
Additional Transfer Techniques: Use of Stretchers and Gurneys
Some equipment, including radiologic equipment, lacks space underneath necessary for a portable floor lift to be used. Other equipment may be located in spaces with no room at the end of the table making it impossible to position a portable floor lift. In such cases, an overhead track lift, either permanently mounted or free-standing, may provide access to the equipment. However, metal components of these overhead lifts may not be compatible with some radiologic technologies.
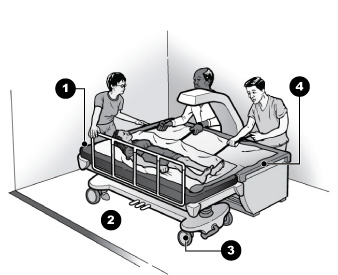
When it is not feasible or possible to use a lift, another option is an adjustable-height stretcher or gurney (a table that is on wheels) that can be raised or lowered to the height of the exam table or surface. This approach involves a two step process in which the patient must transfer from their wheelchair to the stretcher, usually in a different space or area away from the equipment, and then from the stretcher to the table or surface. As many stretchers do not lower to 17" to 19" above the floor, an assisted transfer with a lift may be required to get the patient onto the stretcher. Stretchers that can be lowered to this range of typical wheelchair seat heights allow individuals capable of independent transfers a choice to do so if they prefer. Once the stretcher is positioned next to the equipment and set at the right height, many people will require assisted transfers utilizing devices such as transfer boards or slip sheets to get onto the table or surface.
Assisted Transfer to Stretcher Utilizing a Portable Floor Lift
- Adjustable height stretchers facilitate transfer onto radiologic equipment with a table surface. Assisted transfers from a wheelchair may require use of a lift.
- Open space under stretcher allows close positioning of lift for transfer.
There are many types of radiologic technologies and equipment associated with them, including MRI, x-ray, CT scan, bone densitometry, mammography, and ultrasound. Most of these technologies require the patient to lie on a flat surface that is part of the equipment. The accessibility issues related to transfer to the surface are similar to those addressed previously under Examination Tables and Chairs. However, because the technology is often integrated into the table, the table may not be able to be lowered sufficiently. In these cases, use of a patient lift or another transfer and positioning technique is particularly important for access to this equipment.
Many radiologic technologies also require the patient to keep still, which may be very difficult for some individuals with a mobility disability, including those with spasticity, tremor, or other condition. Patients may need a staff person to support them with pillows, rolled up towels, wedges, or by holding onto them.
Assisted Transfer to Densitometer Utilizing a Stretcher
- Set stretcher height to be level with table surface for lateral transfer.
- Adequate floor space to maneuver and position stretcher.
- Stretcher locked in place to prevent movement during lateral transfer.
- Slip/slide sheets, boards, or other aids assist with lateral transfers.
A mammography exam typically requires the patient to stand up. Individuals who use wheelchairs will need to have an exam while staying in their wheelchair. The mammography machine will need to adjust to their height and accommodate the space of the wheelchair. People who walk with a mobility device or who cannot stand for prolonged periods of time may need to sit in a chair with adequate support, locking wheels, and an adjustable back and, like people who use wheelchairs, need the machine to adjust to their height once seated. Additionally, some patients may need support to lean forward.
Accessible Mammography Machine
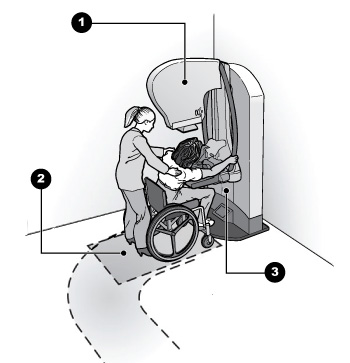
- Unit pivots to multiple angles and adjusts in height for seated patients.
- It is best to position equipment to allow both front and side approaches; for some patients a side or angled approach may be better for positioning at the camera unit and plate.
- Clearance is needed beneath the camera unit and plate to allow people using wheelchairs and other mobility devices to pull up to the equipment.
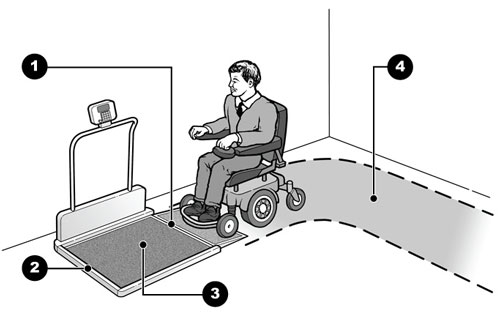
A patient's weight is essential medical information used for diagnostics and treatment. Too often, individuals who use wheelchairs are not weighed at the doctor's office or hospital, even though patients without disabilities are routinely weighed, because the provider does not have a scale that can accommodate a wheelchair. Medical providers should have an accessible scale with a platform large enough to fit a wheelchair, and with a high weight capacity for weighing an individual while seated in his or her wheelchair. Other options may include a scale integrated into a patient lift, hospital bed, or exam table.
Accessible Scale
|
The previous information provides guidance on the ADA's requirement to provide accessible health care to individuals with mobility disabilities as well as illustrated examples of accessible medical equipment, room and office configurations, and lifting and transfer equipment and techniques. This guidance, when applied and adapted to the specific needs and circumstances of individual health care providers, can help ensure that people with mobility disabilities have an equal opportunity to receive accessible health care services.
Staff Training
A critical, but often overlooked component to ensuring success is adequate and ongoing training of medical practitioners and staff. Purchasing accessible medical equipment will not provide access if no one knows how to operate it. Staff must also know which examination and procedure rooms are accessible and where portable accessible medical equipment is stored. Whenever new equipment to provide accessible care is received, staff should be immediately trained on its proper use and maintenance. New staff should receive training as soon as they come on the job and all staff should undergo periodic refresher training during each year.
Finally, training staff to properly assist with transfers and lifts, and to use positioning aids correctly will minimize the chance of injury for both patients and staff. Staff should be instructed to ask patients with disabilities if they need help before providing assistance and, if they do, how best they can help. People with mobility disabilities are not all the same - they use mobility devices of different types, sizes and weight, transfer in different ways, and have varying levels of physical ability. Make sure that staff know, especially if they are unsure, that it is not only permissible, but encouraged, to ask questions. Understanding what assistance, if any, is needed and how to provide it, will go a long way toward providing safe and accessible health care for people with mobility disabilities.
For more information about the ADA, please visit our website or call our toll-free number:
ADA Website
archive.ada.gov
ADA Information Line
800-514-0301 (voice)
833-610-1264 (TTY)
24 hours a day to order publications by mail
M-W, F 9:30 a.m. – 5:30 p.m., Th 12:30 p.m. – 5:30 p.m. (eastern time) to speak with an ADA Specialist.
All calls are confidential.
For more information about Section 504,
visit the Department of Health and Human Services Office for Civil Rights website at:
www.hhs.gov/ocr.
A list of HHS OCR regional offices near you can be found at:
https://www.hhs.gov/ocr/about-us/contact-us/index.html.
Section 504's requirements for new construction and alterations to buildings and facilities are found at 45 C.F.R. Part 84, Subpart C for recipients of federal financial assistance. The regulations are available at:
www.hhs.gov/ocr/civilrights/resources/laws/index.html.
For persons with disabilities, this publication is available in large print, Braille, audio tape, and computer disk.
July 22, 2010
The Americans with Disabilities Act authorizes the Department of Justice (the Department) to provide technical assistance to individuals and entities that have rights or responsibilities under the Act. This document provides informal guidance to assist you in understanding the ADA and the Department's regulations.
This guidance document is not intended to be a final agency action, has no legally binding effect, and may be rescinded or modified in the Department's complete discretion, in accordance with applicable laws. The Department's guidance documents, including this guidance, do not establish legally enforceable responsibilities beyond what is required by the terms of the applicable statutes, regulations, or binding judicial precedent.
Access To Medical Care For Individuals With Mobility Disabilities (PDF Version)
Originally issued July 22, 2010, last updated February 28, 2020